At the Happier Lives Institute, we think that providing free psychotherapy for people with common mental health challenges living in low-income countries is a good idea.
In fact, we think it’s one of the most cost-effective ways to increase wellbeing globally. The only organisations currently occupying our “top charity” spots (StrongMinds and Friendship Bench Zimbabwe) provide psychotherapy at scale and low cost in sub-Saharan Africa. We also discuss ACTRA at the end of this blog.
But many people we talk to find this strange. Some of us did too in the beginning. Isn’t mental health a rich world issue? And isn’t it sort of strange to provide therapy to someone when they’re impoverished and they’re struggling to find enough food to eat? Isn’t it just better to focus on reducing poverty, rather than mental illness, if you want to improve the lives of those in poverty?
These questions are reasonable. Indeed, it seems like there would be something perverse about teaching people to tolerate what should be intolerable circumstances. But we don’t think this is the right way to think about it for some simple reasons.
How therapy improves the lives of the poor
- More therapy means less depression which leads to less poverty.
- Depression is profoundly painful and easily treatable, and that alone is reason enough to act – at HLI, we want to reduce misery, and poverty is not the only source of misery.
- Our research finds that providing therapy to treat depression is more cost-effective at improving wellbeing than cash transfers sent to people living in poverty (who aren’t necessarily depressed).
- Therapy isn’t just useful as a tool to treat depression, it can effectively tackle a wide range of problems – including reducing criminal behaviour for at least 10 years!
How poverty and depression are often interlinked
Poverty and common mental health conditions are tightly interlinked. In a 2020 paper that inspired some of our early work at the Happier Lives Institute, Matthew Ridley and colleagues summarised the relationship between material and psychological scarcity.
They found that negative economic shocks (like a currency crisis) led to higher rates of mental illness. So more poverty → more mental illness. But encouragingly, they presented some initial evidence that:
- Reducing poverty (with cash transfers or anti poverty programmes) led to improved mental health.
- That treating common mental health conditions like depression improved economic outcomes like days worked.
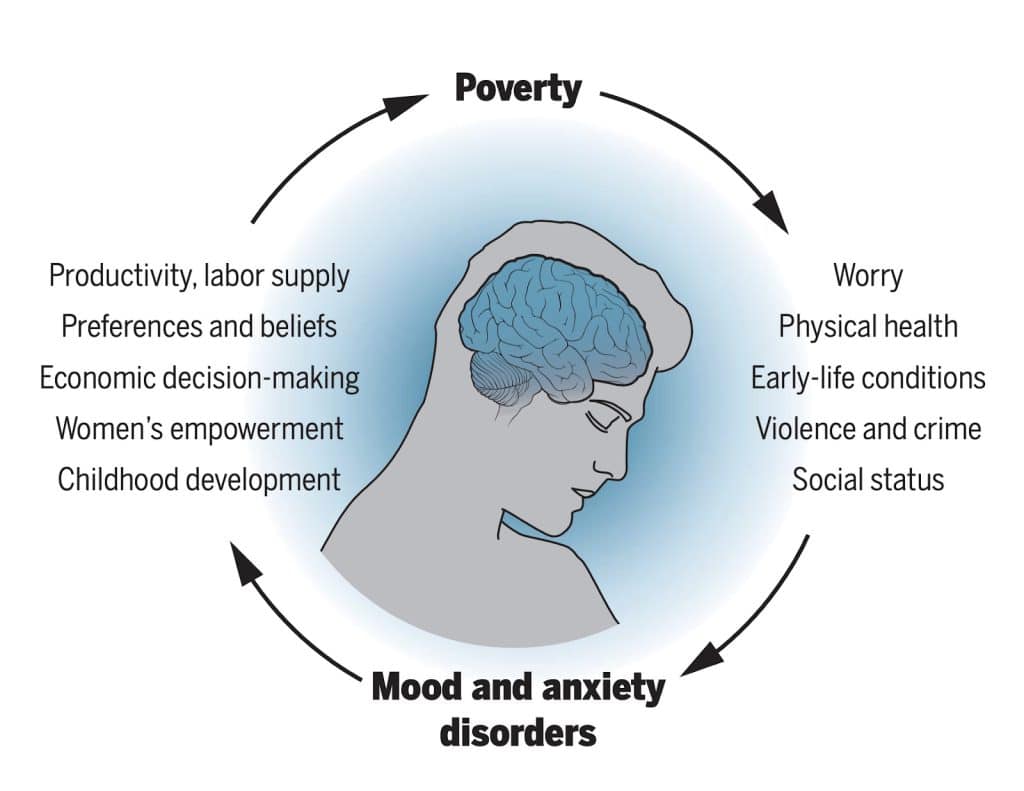
Source: Ridley et al. (2020)
However, since the publication of the review even more evidence has come out supporting this link!
Sending cash, increasing happiness
In part inspired by Ridley et al., we set out to do a full systematic review and meta-analysis of the effect of cash transfers on mental wellbeing. We found that cash transfers have a real and long-lasting effect on the mental wellbeing of their recipients.
So decreasing poverty → decreasing mental illness and increasing mental wellbeing.
Treating depression, improving productivity
Likewise, another meta-analysis by Lund et al. (2024) rigorously summarised the available effect of treating mental health conditions.
They found that mental health interventions increased labour market outcomes like employment, time spent working, and capacity to work. Concretely, they found that psychotherapy interventions like the ones StrongMinds and Friendship Bench Zimbabwe deliver increase the number of days working by ~10%!
We should treat depression because it’s bad
It’s reassuring that treating common mental health disorders like depression can potentially reduce poverty. But the reason we should treat depression is because depression is terrible. It’s synonymous with suffering. We can coherently say “He’s happy but he’s poor”, but “She’s depressed, but happy” is not a sensible sentence.
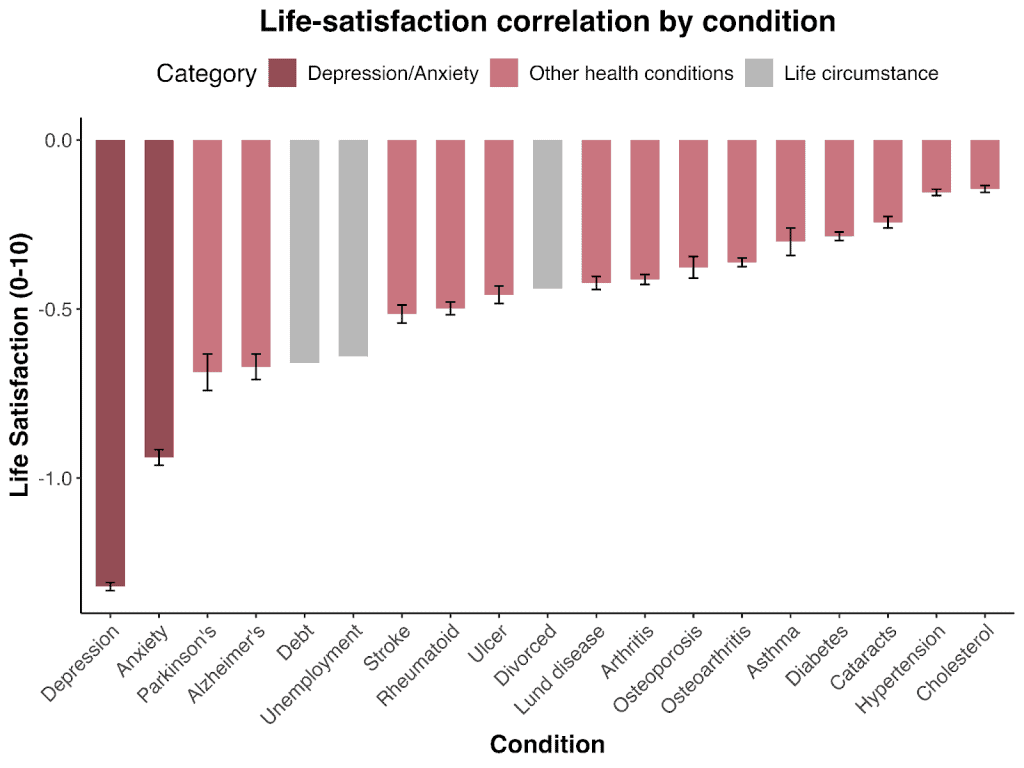
Depression is one of the worst things that can happen to you. See the bar chart reproduced, from HRI, 2020, which looks at various of life’s misfortunes, with the negative impact in terms of a 10-point scale (N.B. this was from European data)
Yet despite the prevalence of common mental health disorders like depression or anxiety (they afflict 4-5% of the world), they receive very little funding in low income countries. These disorders only receive ~1% of governmental health spending in low- and middle-income countries (LMICs) and 0.3% of health-directed international assistance. The low investment in mental healthcare shows.
In low- and middle-income countries (LMICs), only 13.7% of people with mental illness receive treatment. This figure is 10.8% for anxiety, of which 2.3% are considered “potentially adequate”, and 8% for depression (3% adequately treated).
All these numbers are from before the aid cuts we’ve seen in 2025, so this will be even worse in the near future.

Therapy works – but it’s no magic bullet
If you speak to people in the global north about their personal experiences of therapy, you get mixed views. Some people say it was life-changing for themselves or people they know. Other people say they had bad experiences, and point to friends who have tried many things and are still depressed.
In a sense, both groups are correct: therapy doesn’t work for everyone, but it does work for most people. It reduces most people’s symptoms, and in nearly half of cases it cuts symptoms by more than half. Therapy is also better than drugs because the benefits last longer. Some people may think mental health treatments are bad because they don’t cure everyone, but medical science cannot cure all physical health ailments either.
Why funding therapy in low-income countries is impactful
And after talking to a number of experts, including in the charities themselves, we think it may work even better in low-income contexts. This is because a crucial ingredient of therapy is psycho-education about mental health: informing people that depression and anxiety are real health problems that can be addressed. People in the global north are now very aware of mental health – but that’s a radical change over the last couple of decades.
In contrast, organisations like StrongMinds and Friendship Bench are often teaching people about mental health for the first time, so there is more beneficial psychoeducation that can happen. From our site visits, we heard first-hand from those charities’ clients about the intense relief they felt when they were able to put a label on what was going on in their heads, and that they could get better, rather than they were broken and would feel that bad forever.
But it’s not just that therapy works, it can be delivered for very little cost by trained volunteers. This leads to a modest loss in effectiveness (~36% smaller), compared to being delivered by professionals with years of training. It’s enough to make me wonder if richer countries have the wrong idea about how to treat common mental health conditions.
Charities we recommend for improving mental health in low income countries
We recommend two charities delivering talk psychotherapy to treat depression and common mental health conditions in Africa: Friendship Bench Zimbabwe and StrongMinds. They can provide therapy cheaply because they primarily rely on volunteers that are trained for several months instead of professionals who go through years of schooling.
While therapy is somewhat less effective when delivered by non-experts, it’s profoundly cheaper. Friendship Bench Zimbabwe provides an average of one to two sessions of Problem Solving Therapy per patient for $17. StrongMinds provides an average of five to six sessions of group Interpersonal Psychotherapy for $45.
Programmes like this can remit depression symptoms for a full year for eight out of 20 people. And one in 20 are still depression-free after seven years3.

Reducing poverty or treating depression, which one’s better?
One increasingly popular way to help those in poverty is cash transfers. It’s tempting to say that cash transfers reduce poverty, and therapy reduces depression, and then ask “so, what’s better, reducing poverty or depression?”
To be clear, this is a false dichotomy. This is because, as we’ve argued above, there is a cyclical relationship between poverty and mental illness. Cash transfers reduce poverty and improve mental health. Therapy reduces poverty and improves mental health.
However, there is a real question, and a choice to make, about which intervention has the greatest impact for the money that goes in: cash transfer or providing therapy (or something else)? Which has the highest wellbeing return on investment?
This is a question we’ve now spent years looking at. We’ve done and published systematic reviews and meta-analyses of the cost-effectiveness, in low-income countries, of both cash transfers and therapy for depression.
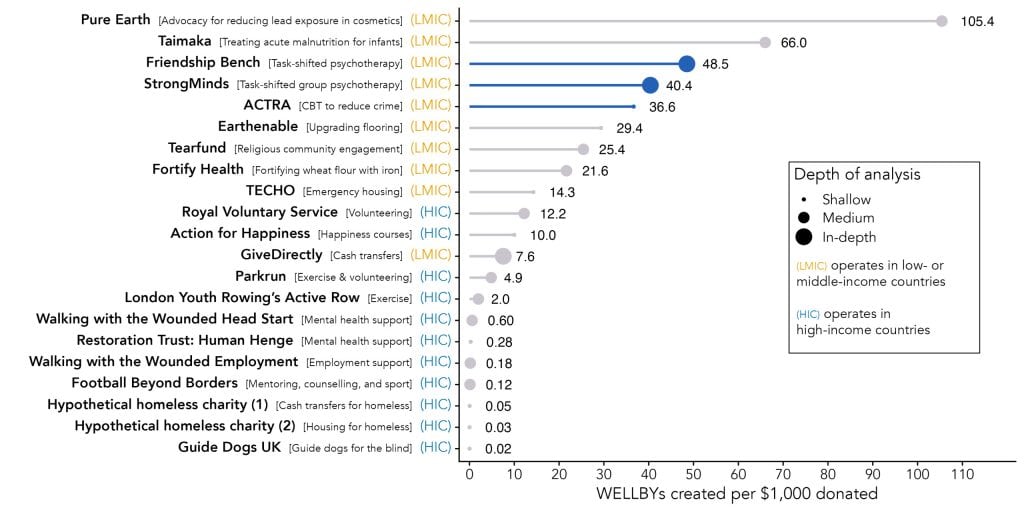
We find that psychotherapy is, perhaps surprisingly, around five to six times more cost-effective than cash transfers! This difference is driven by the costs. To be clear, a $1,000 cash transfer has about 5x the effect on the people who receive it than the $50 worth of therapy does. But that $1,000 cash transfer also costs about 25x more, per person, to provide than the therapy does. This is how the therapy ends up being about five times more cost-effective.
We should emphasise these interventions target different groups: cash transfers go to people who are very poor (and may or may not be depressed), therapy is provided to those diagnosed with depression (who are also very poor). We are often asked about this, but we have not looked at the cost-effectiveness of providing therapy to poor, non-depressed people; this would be of academic interest only, seeing as providing therapy to depressed people will clearly be more cost-effective than providing it to non-depressed people.
Therapy: it can also tackle crime!
Like a commercial that won’t end, we have more to say about therapy. It doesn’t just address poverty, and provide a scalable treatment for depression and anxiety, it may also … reduce crime?
We’ve provided more shallow evaluations of ACTRA in Colombia, which use cognitive behavioural therapy to prevent crimes from happening through decreasing impulsivity, anger issues, and identification as an outcast or criminal.
ACTRA is currently developing a programme based on a large well designed RCT which found some remarkable results of combining cash and CBT to reduce crime in offenders. Ten years after it was delivered, the programme found large effects on the criminality and the mental wellbeing of its recipients: 34 fewer reported thefts a year for the recipients, and a substantive boost to mental wellbeing. After accounting for programme expenses, the authors concluded their results imply a cost of roughly $1.50 per crime avoided. Notably, these effects were surprisingly durable, showing practically no signs of decay after ten years. The difference is that ACTRA will deliver it in Colombia, and they do not use cash transfers, instead only using the CBT component. We haven’t evaluated their programme since it hasn’t been finalised yet, but we think they’re an organisation to watch out for!
The lesson here is that a crucial way to improve people’s lives is to help them learn and reflect, understand themselves and their emotions better, and engage differently with the world. This is, in general, what therapy does, so it’s perhaps unsurprising it can help with things as seemingly different as mental illness and criminal behaviour.
Want to know more? Or better yet, do more?
- Learn more: Visit our charity evaluations page for detailed reports on all of the topics discussed.
- Stay informed: Sign up to our (regular but not too regular 😉) newsletter for updates and new insights.
- Donate: Fund very cheap and effective psychotherapy through StrongMinds, Friendship Bench Zimbabwe, or even ACTRA.
- Advocate: Share these findings. Mental health matters more than many expect.
Featured image credit: Friendship Bench Zimbabwe.